






Click the links below to access content on each subject area pertaining to Airway Management.
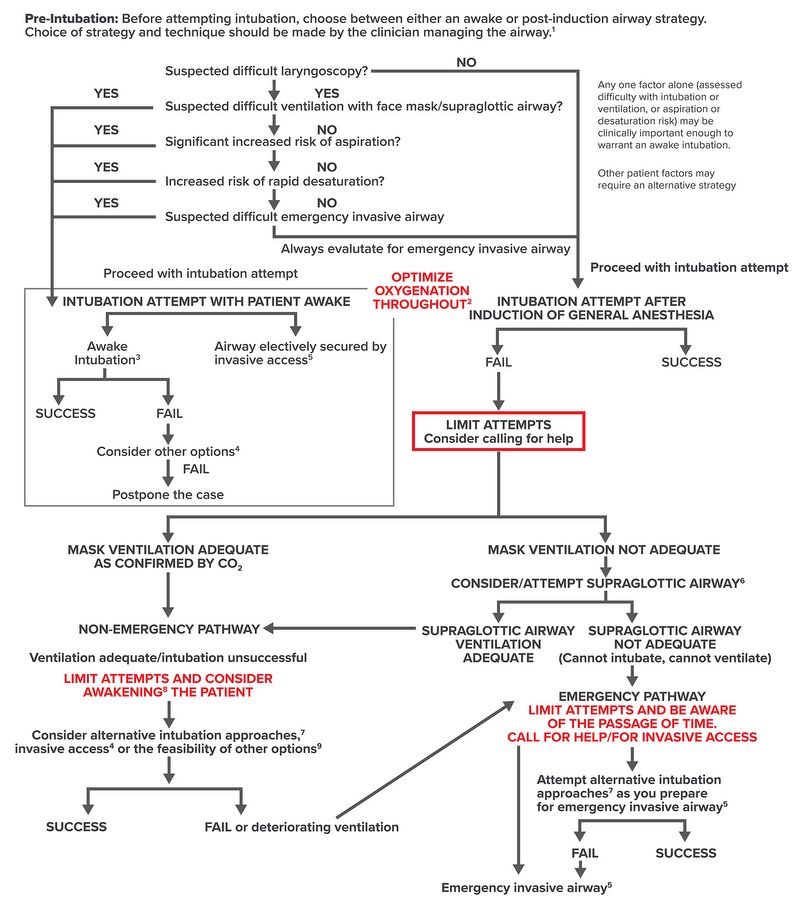
→ Mask ventilate (Adequate) → Non-emergency pathway
→ Mask ventilate (Inadequate) → Supraglottic airway
→ Supraglottic airway (Inadequate)
CANNOT INTUBATE/ CANNOT VENTILATE
Invasive access should be attempted